Sites Offer Key Insights to Challenges of Risk-based Methodologies Associated with ICH E6 (R2)
In April 2018, The Avoca Group and The Association of Clinical Research Professionals (ACRP) co-sponsored a one-day program, the 2018 Quality Congress, in conjunction with the ACRP Annual Meeting (ACRP 2018). This full-day event offered participants – clinical research professionals from CROs, sponsor organizations, and sites – a unique view of the changing clinical trial landscape with a focus on quality in clinical trial execution.
Although the FDA released risk-based monitoring guidance in 2013, it wasn’t until the release of ICH E6 (R2) in 2016 and its focus on risk-based monitoring that the industry began to shift from 100% SDV to risk-based approaches.
Because of R2’s focus on risk and the need to comply with these guidelines, the majority of conversations held at the Quality Congress centered around risk-based methodologies. These discussions highlighted frustrations felt from all sides of the clinical trial landscape.
The two most commonly voiced frustrations were unclear communication and lack of transparency. Unclear communication, we heard, was not the result of bad intentions. Instead, it became quickly apparent that the industry as a whole does not have a clear understanding or definition of risk-based monitoring.
Key monitoring-related terms often include risk-based monitoring, central monitoring, site monitoring, on-site monitoring, and remote (or off-site) monitoring. Each of these types of monitoring comes with different roles and responsibilities. For efficient, effective monitoring, we need to ensure that all players in the monitoring of the clinical trial understand what is expected from both the monitoring and their role (Figure 1).
Click image to enlarge
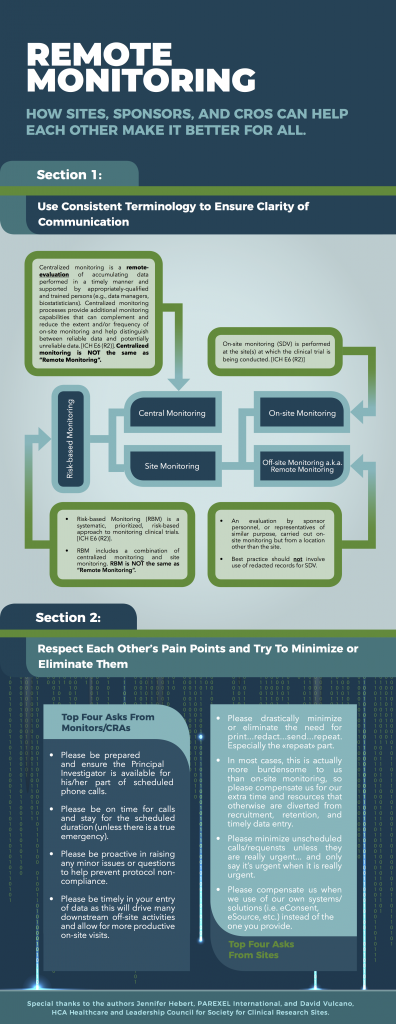
Figure 1. David Vulcano, HCA Healthcare and Leadership Council for Society for Clinical Research Sites, and Jennifer Hebert, PAREXEL, created this diagram to define and outline the relationship between the types of monitoring.
The issue around lack of transparency was related to expectations for risk-based monitoring plans. Sites noted that the first step in reducing frustration and increasing site efficiency is understanding what is expected at monitoring visits, while sponsors noted that, to avoid a focus solely on the datapoints and main areas in the risk-based monitoring plans, they do not frequently share the plans with sites.
However, the shift toward risk-based monitoring has also moved the responsibility for quality control check from CRAs to the sites themselves. When CRAs were responsible for the quality control check with 100% SDV, the sites could be assured that the data they entered was of high quality because of the second set of eyes reviewing it.
With risk-based monitoring approaches, the ability to review the study monitoring plans would allow sites to focus their quality control efforts on the datapoints and/or focus areas that will not be checked again by the Sponsor. This issue was an example of a clear misunderstanding that, when discussed openly, seemed to have a very rational outcome: risk-based monitoring plans would be shared with sites so they can implement quality control steps where most appropriate.
Conversations like these increase industry-wide quality and efficiency in clinical trial execution. It is our hope that conversations of this nature will be ongoing as The Avoca Group continues to involve sites in the development of quality tools within the Avoca Quality Consortium®.